Breast Cancer: Symptoms, Stages & Treatment Options
Two FDA-approved gene therapies are currently available in the U.S. for transfusion-dependent beta-thalassemia: Casgevy for patients age 12 and older, and Zynteglo for adult and pediatric patients who require regular red blood cell transfusions.
Breast cancer is not one single disease. Treatment decisions depend on the cancer’s stage, grade, and biomarker profile, especially hormone receptor status and HER2 status. NCI notes that breast cancer staging now combines TNM stage with grade and biomarker status, and all breast cancers are tested for biomarkers such as estrogen receptor, progesterone receptor, and HER2 to help guide treatment.
Key Facts
Breast cancer can begin in different parts of the breast and may behave differently from one person to another. Some types are hormone-driven, some overexpress HER2, and others are triple-negative, meaning they lack estrogen receptors, progesterone receptors, and high HER2 expression. These differences are important because they influence treatment options and prognosis.
The stage also matters. Stage 0 is a non-invasive form such as ductal carcinoma in situ, while stages I through IV reflect increasing spread. NCI explains that stage is based on tumor size, lymph node involvement, spread to other parts of the body, grade, and biomarkers.
Symptoms
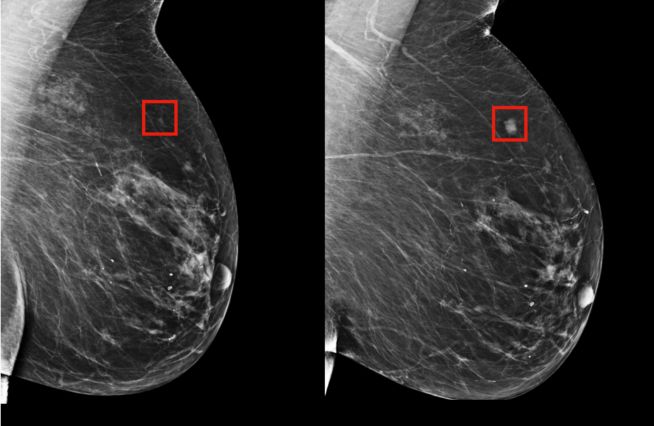
The most common breast cancer symptom is a new lump or mass, but not every breast cancer presents this way. Other breast or underarm changes should also be checked.
- A new lump or thickening in the breast or underarm
- Change in breast size or shape
- Dimpling or puckering of the skin
- Nipple turning inward
- Nipple discharge, especially if bloody
- Red, scaly, or swollen breast or nipple skin
- Breast skin that looks like orange peel
- Ongoing breast change that feels different from usual
Diagnosis
Diagnosis usually begins with imaging and biopsy rather than symptoms alone. Breast cancer evaluation also includes biomarker testing, since treatment planning depends on the tumor’s biology as well as its stage. All breast cancers are tested for hormone receptors and HER2, while some may also be evaluated for markers such as Ki-67 or multigene features depending on the clinical situation.
Breast cancer staging uses the TNM system. Final stage is not based only on tumor size. It is determined using tumor size and spread, lymph node involvement, distant spread, grade, and biomarker status.
- Stage 0: Very early non-invasive disease, often called carcinoma in situ.
- Stage I: Small invasive cancer with little or no lymph node spread.
- Stage II: Larger tumor and/or limited spread to nearby lymph nodes.
- Stage III: Locally advanced disease with more extensive lymph node involvement or spread into nearby tissues.
- Stage IV: Metastatic breast cancer, meaning the cancer has spread to distant parts of the body.
Why grade and biomarkers belong in this section
Grade helps describe how abnormal the cancer cells look and how fast they may grow. Biomarkers such as ER, PR, and HER2 help determine both stage grouping and treatment strategy. This is also the right place to explain common subtype language like HER2-positive, hormone receptor-positive, and triple-negative breast cancer.
| Treatment Type | How It Is Used |
|---|---|
| Surgery | Often used in early-stage disease to remove the cancer from the breast and sometimes lymph nodes. |
| Radiation Therapy | Often used after surgery to reduce the risk of cancer coming back in the treated area. |
| Chemotherapy | Used in some early-stage and metastatic settings, especially when the cancer is higher risk or less likely to respond to hormone therapy alone. |
| Hormone Therapy | Used for hormone receptor-positive breast cancers. |
| HER2-Targeted Therapy | Used when the cancer is HER2-positive. |
| Immunotherapy | Used in selected settings, including some triple-negative breast cancers. |
| Clinical Trials | May matter in both early-stage high-risk disease and metastatic disease, especially when standard options are limited. |
Triple-negative breast cancer
Triple-negative breast cancer does not have ER, PR, or high HER2 expression, so hormone therapy and HER2-targeted therapy are not the main treatment tool.
HER2-positive breast cancer
HER2-positive cancer has high HER2 activity and may respond to HER2-targeted treatment.
Side effects depend on the treatment used, not just the cancer diagnosis. Surgery, radiation, chemotherapy, hormone therapy, targeted therapy, and immunotherapy all have different side-effect patterns, which is why readers should be guided into treatment-specific pages.
- What side effects may happen during treatment
- When to contact the care team
- How caregiver support can help
- Links to treatment-specific support pages
- Downloadable question list for appointments
Clinical Trials
Clinical trials should be framed as one possible next step, not the default next step. They may be especially relevant when the cancer is high risk, metastatic, recurrent, HER2-positive with changing options, triple-negative, or no longer responding to standard treatment. NCCN and NCI patient resources both support using subtype and stage to guide decision-making and trial discussions.
Questions to Ask Your Care Team
What type of breast cancer do I have?
What stage is my cancer?
What grade is it?
Is it ER-positive, PR-positive, HER2-positive, or triple-negative?
Which treatments do you recommend first, and why?
Will I need surgery, radiation, chemotherapy, hormone therapy, targeted therapy, or immunotherapy?
Should I consider a clinical trial at this stage?
What side effects can I expect?
What should my caregiver or family watch for?
What are the key decisions I need to make in the next few weeks?
FAQ
Is gene therapy available for beta-thalassemia?
Yes. In the U.S., FDA-approved gene therapy is available for transfusion-dependent beta-thalassemia through Casgevy and Zynteglo, with different label wording and age scope.
Does it help patients who need regular transfusions?
Yes, that is the main setting where it is used. Casgevy is approved for transfusion-dependent beta-thalassemia, and Zynteglo is approved for patients with beta-thalassemia who require regular red blood cell transfusions.
What is the difference between Casgevy and Zynteglo?
Casgevy is a gene-editing therapy, while Zynteglo is a gene-addition therapy. Both use the patient’s own stem cells, but they are different products with different manufacturing strategies and label wording.
What are the main risks?
The main risks are the risks of myeloablative conditioning, including severe low blood counts, infection, fertility concerns, and the need for careful hospital-based recovery and long-term follow-up.
treatment and follow-up?
The treatment path includes evaluation, stem-cell collection, manufacturing, conditioning, infusion, marrow recovery, and long-term follow-up. There is not one universal timeline that fits everyone, because recovery and logistics vary by patient and center.
When is transplant still preferred?
Transplant may still be preferred when donor availability, center expertise, disease severity, and the overall risk-benefit balance make it the stronger option. This choice is individualized and should be reviewed at a specialist center.
Medical Disclaimer & Source References
© BEIJING BIOTECH.
Clinical Sources: NCCN, ASCO, ACS, ESMO, CSCO, CACA, ChiCTR.
Medical Note: This page provides general information and does not replace physician evaluation, diagnosis, or treatment planning.